
Medication for Depression
Is depression an illness?
There is some debate within the mental health community about the biological basis of depression. Many who approach this issue from a medical perspective would describe depression as a disease. In my view, there could be some truth in this and certainly it may help many sufferers to come to terms with their depression if they feel it is acknowledged as physical condition, particularly if it is described as being associated with an imbalance of certain brain chemicals over which they have no control, as is often the case.
I think we still have to ask however whether this imbalance causes the depression or is something which arises as a result of depression. My own view is that some people are undoubtedly predisposed to a risk of depression (just as some people are predisposed to risk of coronary heart disease, based on hereditary (genetic) factors. However, not everyone was such a predisposition experiences a problem. In the case of heart disease for example, it very much depends on your diet and lifestyle.
Almost 50 million prescriptions for antidepressants were issued in the U.K. in 2011, a rise of 9% over 2010
At the end of the day it may not matter who is right. What may be more important is how we respond to the symptoms of depression. As a counsellor and psychotherapist I know from my own experience over 19 years of therapy very often helps. I also acknowledge however that medication can play an important role and that often, a combination of medication and therapy is more effective than either on their own. In this section of my website I provide some information about medication and offer some explanations as to how we think it might work. I say "might work" because I have yet to see truly convincing evidence that we understand this process completely.
The Biological Basis of Depression
In order to understand antidepressant medication, we need to know a little about what we think happens in the brain when we are depressed
When we are depressed, physical changes take place within our bodies. The most important of these take place within the brain and believe it or not, the gut. It is on this basis that depression is considered a physical illness, rather than merely something psychological or something that exists only in the imagination or perception of the sufferer. It is perhaps important to remember this if you, or someone you know, is diagnosed as having depression. Remember, one cannot simply think oneself out of it! There are real and tangible changes taking place in the physiology of someone suffering from clinical depression. Back to Top
The Brain, Neurons & Synapses
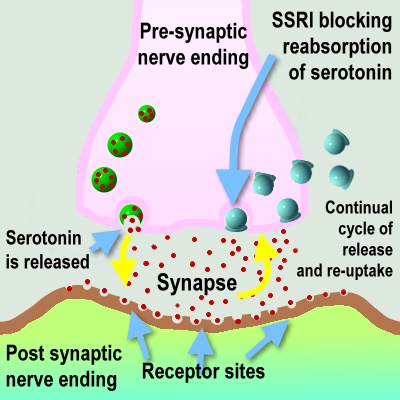
Diagram showing a nerve ending and synapse and model of impulse transmission using neurotransmitters which are released and continually subject to re-uptake. Modern antidepressants like SSRIs are thought to work by blocking the reuptake of serotonin, thereby alleviating symptoms of depression. Illustration by the author.
There are something like 10,000 million cells in your brain. Each of the cells has connections to other cells. It is thought that each brain cell may have as many as 25,000 connections to neighbouring cells. Of course, although each cell has the potential to be connected, in practice, these connections are not happening constantly. When connection is made, it is in the form of an electrical impulse which travels down the connections between nerve cells (neurons) at a speed of about 120 mph. This process happens every time we think a thought or decide to move a muscle. It also happens every time something automatic and unconscious happens, for example, breathing air in and out, digesting a meal or releasing a hormone.
The neurons that carry these electrical impulses contain small gaps called synapses. These are important because they allow electrical activity, and hence brain functioning, to be mediated (or controlled). In order for an impulse (or message) to jump from one neuron across the synapse to another, a number of important enzymes, called neurotransmitters, have to come into play. In total there six different groups of neurotransmitters and each one is specific to a particular type of brain cell. From the point of view of depression, the main neurotransmitters are serotonin (sometimes called 5HT or 5 hydroxytryptamine) and noradrenaline (sometimes called norepinephrine).
It is known that people suffering from depression have low levels of these two neurotransmitters and this is thought to lead to the main symptoms of low mood, low-energy, depressed outlook, disturbed sleep and low drive or arousal. Again, it is worth emphasising that although depression is "in your head" it has very real physical consequences and these are not merely imagined -- they arise out of distinct chemical changes in the brain. Back to Top
So, is Depression purely about biology?
Because depression is associated with low levels of certain important neurotransmitters, it led to speculation about depressing having purely biological causes. Years ago, many doctors believed that depression arose as a consequence of deficiencies in levels of certain of these brain chemicals. In this view, depression might be little more than a physical illness. So, just as diabetes is a disease caused by insufficient insulin production, so might depression be a disease caused by insufficient production of serotonin or noradrenaline.
Such a perspective would have consequences in terms of the potential for us to effectively "inherit" depression, in as much as the characteristic (or "depression gene") might be passed down in families. There was certainly some evidence for this view -- we know, for example, that having a parent who suffers from depression can make it more likely that you also will suffer from depression. However, most clinicians now believe that such a view offers us only a partial understanding of the mechanisms of depression.
Recent advances in neuroscience have been able to prove beyond almost any doubt that these same chemical changes can arise as a result of changes in our environment. Factors such as anxiety or stress, for example, or hormonal changes, can affect neurotransmitter levels. Few doctors now hold to the view that depression is purely a biological disease arising from deficiencies in production of neurotransmitters. The brain is an incredibly complex place and we still understand relatively little about all of its functioning. My own view is that whilst it may be possible to inherit a predisposition (or if you like a potential tendency) to develop depression, the expression of this tendency will very much depend on our environment, nutrition, lifestyle and our life experiences -- particularly those of childhood where our "world view" is being developed. Any potential tendency towards depression can therefore either be reduced or increased, depending upon how we have lived our lives and the views we have developed because of this. This is where talking therapy can have an important role, helping people become aware of their perspectives, many of which might be unhelpful or inappropriate and supporting them to adopt new and more adaptive ways of thinking and being in the world.
How Antidepressants Work
Taking a purely biological point of view, it seems fairly obvious that if depression is associated with shortages of certain key neurotransmitters then the "cure" for depression ought to be to address this deficiency, rather like the cure for scurvy is to supplement the diet with vitamin C. Although this is far from being the whole picture, this is pretty much how we think antidepressants work. The exact process is of course rather more complicated and research is still continuing in order to establish a more complete picture.
After a nerve impulse has been carried across the synapse by a neurotransmitter like serotonin (see "the brain, neurons and synapses" above for an explanation of this), the neurotransmitter is either broken down by enzymes and removed or taken back up again into the nerve ending and recycled for future use - a process known as re-uptake.
Many of the main antidepressants work by blocking this recycling process. Antidepressants such as Prozac (fluoxetine) and Seroxat (paroxetine) are known as SSRIs -- Selective Serotonin Reuptake Inhibitors. To think of such medication as merely being stimulants is therefore to grossly oversimplify their mode of action. Contrary to popular belief, SSRIs are not "happy pills". They do not directly enhance mood and they do not, of themselves, promote happiness. At best, they may give you the capacity to once again behave and think in ways that can help you to function more normally.
Some antidepressants, such as the examples mentioned above, work specifically on serotonin whilst others work on noradrenaline and a few (mirtazapine, for example) work on both. Venlafaxine works on three neurotransmitters (including dopamine) at high enough doses.
When we are depressed we don't feel like doing the things that would be good for us and moreover our performance (for example at work or in school/college) is compromised. This means we don't achieve such good results and this can tend to lead to still greater levels of depression. One of the main benefits of antidepressants is that they can break this so-called "cycle of depression".
Although antidepressants don't actually change our world, they can at least give us the energy and perhaps just enough enthusiasm to take the first steps towards re-engaging with our lives. If we start to see better outcomes from our efforts in life then we will tend to feel better about life and perhaps ourselves, which will boost our confidence and lead to still greater levels of success and enjoyment. In severe cases of depression, the sufferer can be almost physically incapacitated from undertaking everyday tasks and may start to cope so badly with life that death seems as if it is the only viable alternative. In such examples antidepressants can quite literally be lifesavers.
A Case Example
One client I worked with had very low levels of assertiveness and because of this was often treated very badly by friends, family and work colleagues. This led to her becoming really rather depressed, which meant that she tended to avoid interactions with other people whenever possible, lowering further still her confidence and her ability to deal with social situations. She was becoming increasingly withdrawn. Whilst the counselling helped her to understand how she was contributing towards her own distress by having so low an opinion of herself, the antidepressants helped her to feel well enough to start to re-engage with people and to put into practice some of the ideas and life skills she was learning in therapy. By the time the medication was slowly withdrawn after her depression had lifted, she had firmly established new patterns of behaviour and relationships. She was easily able to continue this new and more useful way of being, therefore removing the need for further medication.
The Disadvantages of Antidepressants
Many people I know would say that when you are profoundly depressed, there are no disadvantages to taking something that makes you feel better. Certainly I know many clients whose lives have been transformed by taking the right antidepressant. Having said that, no medication is without its problems. There are no "magic bullets".
The main problems are firstly, finding the right antidepressant and secondly, side-effects. Antidepressants seem to help about half of the people who take them and different antidepressants work better with some people than others. The process of matching the right medication to the person is far from a precise science and one psychiatrist I know will admit that it often comes down to luck and guesswork. Having said that, the choice of antidepressant is usually informed by the exact nature of the symptoms experienced. For example, some antidepressants are associated with a lowering of anxiety, others with sedation (useful in cases of severe insomnia) and still others with a very low risk in case of overdose. It is also important that the antidepressant is prescribed at the right dosage and there is some evidence to suggest that some GPs err too much on the side of caution here. All antidepressants have a slow onset of action, with most taking at least two weeks to have any beneficial effect. It is usually a month before the optimum level of efficacy is reached and up to six weeks may be required for full effect.
Side Effects
Although modern antidepressant choices have far fewer side-effects than was the case with some of the older, so-called, tricyclic antidepressants, this can nevertheless still be a problem in some cases. Drug manufacturers are increasingly designing antidepressants to have a highly specific mode of action, with only the selected neurotransmitter targeted. SSRIs, for example, are designed to be selective of serotonin but even so, this neurotransmitter also controls digestion, appetite, blood pressure, temperature control and sleep regulation. This is why SSRIs can sometimes be associated with unwanted effects such as sweating, weight gain and insomnia.
In practice, and for most people, the disadvantages of these unwelcome side-effects are far outweighed by the advantages. Nevertheless, many patients do stop taking their medication in the first few days when the side-effects (if they occur at all) are most likely to be at their worst. It is worth remembering that problems with side-effects usually decline after three to five days and most modern antidepressants are well tolerated.
Other antidepressants impact on other neurotransmitter systems as a side effect of targeting those involved in depression. Zispin (mirtazapine) for example impacts on serotonin and noradrenaline levels but also affects the histamine system, meaning that it initially causes significant drowsiness in many patients. Against this, mirtazapine rarely has an adverse effect on sexual desire or performance, a characteristic unfortunately associated with some of the SSRIs.
All the older tricyclic antidepressants are much less specific and so can potentially have a broader range of unwelcome effects such as dry mouth and blurred vision. Nevertheless, they still have their uses and I have sometimes seen my clients respond well when prescribed this type medication by their doctor, where the more modern alternatives have failed to be of benefit.
Another characteristic to be aware of is that medication can sometimes be so effective as to make you feel that you no longer need to take it. After a time, you can become convinced that your depression is no longer a problem and indeed, it won't be, for as long as you continue to take the tablets! Remember, depression tends to be a longer term illness or condition and this means you may be taking antidepressants for many months, including a period of time during which you are feeling completely "back to normal". One of the most important factors in preventing a recurrence is a continuation of medication beyond the point where all symptoms have disappeared. Often, there is an easily recognisable point in time at which to stop, such as the resolution of problem or a point at which you feel you have come to terms with a situation -- perhaps as a result of counselling.
In other cases, it may be necessary to take medication for extended periods, possibly as long as many years. The point at which you may be ready to stop is something you need to discuss carefully with your GP, and possibly with your therapist. Even then, it is important not to discontinue medication suddenly and your doctor may well discuss a regime for gradually reducing the dosage over several days or possibly weeks, depending on the type of medication and the dosage taken. No antidepressant can cause physicaladdiction, despite what may be claimed in the media or on the Internet. However, you may understandably feel a certain amount of trepidation about discontinuing treatment and coping without it, especially if you have taken it for many months or years. In practice, problems with discontinuation are rare. I myself have encountered only one client (out of the many hundreds that I have seen) who had significant problems whilst he was stopping antidepressant medication.
Remember, if you are uncertain about how well your medication is working, or if you have questions or concerns about dosage, side-effects or discontinuation, you should always speak to your doctor. The information provided here is for general guidance only and is not intended to replace consultation with a medical practitioner.
Use the links below and at the top to skip to a specific section.
Mild Depression
Moderate to Severe Depression
Differences between depression in men and women
Depression facts
Medication for depression (you are here)
Depression symptoms (next page)
Test for depression
Different experiences of depression are discussed on the pages above, together with some of the therapeutic options relevant to each type.